-

- CT multiplanar reconstruction shows a split-fracture of L1 vertebra.

-
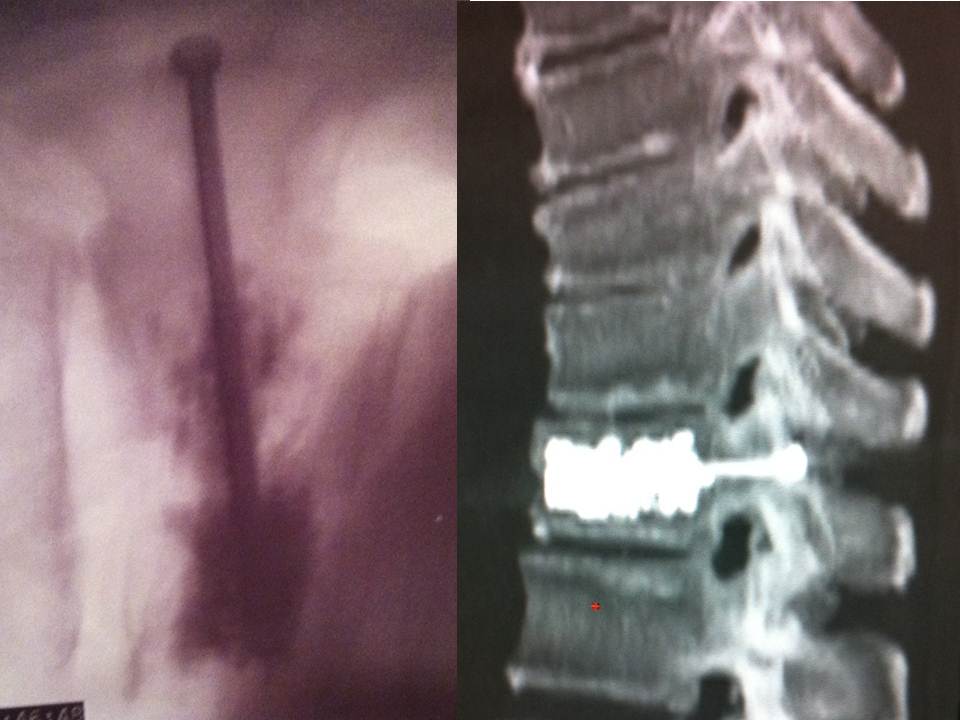
- Following the withdrawal of the cannula , a 4-mm cannulated self-drilling/tapping screw was placed over the Kirschner guidewire.

-
- The CT guidance allowed a perfect visualization of the screw

-
- The trocars are advanced successively under monitoring by CT slices and lateral fluoroscopy

-
- the cement is injected at the level of the anterior fragment of the fracture then the trocar is withdrawn slowly

-
- high radio-opacity makes visualization perfect during vertebral filling (CT and fluoroscopy)
Split fracture of the spine: Combined percutaneous vertebroplasty and screw fixation under CT and fluoroscopy guidance.
A new technique.
Abstract
Objective
The aim of this study was to evaluate CT- and fluoroscopy-guided percutaneous vertebroplasty and percutaneous screw fixation in the management of split burst fracture (Magerl A2).
Materials and Methods
Institutional review board approval and informed consent were obtained for this study. Ten consecutive adult patients were prospectively treated by an interventional radiologist. All these procedures were performed under local anesthesia. . The axial slices permit perfect visualization of the ends of the trocars precisely within the vertebral fracture. The fluoroscopic guidance verifies that the trocars are at mid-height of the vertebra. The trocars are advanced successively under monitoring by CT slices and lateral fluoroscopy. The perfect position and length of the screw is determinate by CT.The post-operative follow-up ranged from 12 to 24 months.
Results
The results obtained match those of the literature in the area of hyperalgesic osteopoenic fractures: The visual analogue scale and Oswestry disability index decreased from 7.5 +/- 1.5 to 2.1 +/- 1.2 and from 65.3 +/- 16.2 to 16.1 +/- 5.0 respectively. CT monitoring revealed satisfactory consolidation of the fracture line. Follow-up CT imaging showed evidence of fracture healing. No evidence of secondary displacement of the fragments, degenerative changes, screw failure or lucency adjacent to screws was noted. All of the results were stable in time and in particular over the long term, at 1 year and 2 years.
Conclusion
Combined percutaneous screw fixation and Vertebroplasty offers an intermediate alternative to the traditional treatments. The brief hospitalization and the speedy return to active life have very interesting economic and social consequences.
Keywords: Vertebroplasty.Percutaneous screw fixation. Burst fracture.Split fracture. Magerl A2.Local anesthaesia. CT and fluoroscopy guidance. Interventional radiology
The percutaneous vertebroplasty procedure was performed for the first time in 1984 by the team of Professor Deramond at Amiens University Hospital Centre in France (1-2). It consists of injecting acrylic cement into the vertebral body in order to consolidate it. The original indication was that of aggressive angioma. The indications have been gradually broadened to include vertebral metastatic disease and then hyperalgesic osteoporotic fractures(3-11). The evolution of the equipment and of the experience of interventional radiology teams has made it possible to expand the group of indications to include stable traumatic fractures.
The treatment of split fractures generally consists of either bed rest and traction or open reduction and internal fixation (Postero-lumbar interbody fusion). Although non-displaced or mild displaced Split fractures can be managed conservatively, internal fixation of these fractures could prevent secondary displacement and allow early weight bearing. However, traditional surgical treatment requires extensive exposure, which may be complicated by infection, blood loss, wound healing problems. Consequently, computed tomography (CT) imaging is routinely used to evaluate Split-burst fractures and plan treatment. The combination of CT and fluoroscopy guidance could reinforce its place in the therapeutic management of vertebral fractures. Indeed, it was shown that this dual guidance allowed to make percutaneous procedures (such as vertebroplasty or posterior arthrodesis of spine) rapid, safe and effective.
Different techniques are necessary in order to improve the safety of the procedure, while a learning curve and good mastery of simple vertebroplasty are imperative before any attempt to use these more delicate vertebroplasties. We describe the approach of minimally invasive procedure with dual CT and fluoroscopic guidance that performed under local anesthesia for better outcome. The purpose of our study was to evaluate CT- and fluoroscopy-guided vertebroplasty and percutaneous screw fixation in the management of Split burst fracture.
To the author’s knowledge, no published reports in the English literature have discussed this type of treatment.
Equipment and method:
All procedures in this study were approved by the Institutional Review Board of our institution. Patients were enrolled after giving written informed consent.
From january 2007 to january 2010 we realized a Single-centre prospective study of 10 consecutive patients without neurologic deficit referred by the trauma departments of our institution for post-traumatic vertebral fracture of class A2 according to the Magerl classification. Procedures were decided only following an interdisciplinary meeting between interventional radiologists and orthopedic surgeons. Step-by-step volume CT over the entire spine made it possible to establish a lesion assessment and to classify the vertebral fracture as split fracture of grade A2 in the Magerl classification (FIG 1).
Description of the technique:
All patients were treated by a senior interventional radiologist (with ten years of experience). After haemostatic control, procedures were performed under surgical conditions of aseptia in an interventional CT room using CT (GE Lightview 8-row MDCT scanner; GE Healthcare, Waukesha, Wis, USA) and lateral fluoroscopy (GE Stenoscop C-arm) guidance. Patients were placed in a prone position on the CT table with a support optionnaly placed under abdomen to decrease lumbar lordosis .
The first part of the intervention was a CT acquisition of the spine with the following parameters: collimation, 8 x 1.25 mm at 100 kV and 250 mAs; rotation time, 0.5 second; pitch, 1.4; field of view, 500 mm, matrix, 512 × 512; standard soft-tissue kernel. Multiplanar reconstructions (with a slice thickness of 1.25 mm) were analyzed on a GE ADW 4.2 workstation to confirm the diagnosis and plan the approach. More precisely, this CT scan allowed to:
– analyze the anatomy of the vertebra and the position of surrounding neurovascular structures.
– determine the best approach so that the direction of screws can be perpendicular to the plane of the fracture line to be fixed. An imaginary line of the proper screw trajectory avoiding the neurovascular structures was drawn on the CT image for guidance: a skin entry point was thus determined.
– and calculate the optimal length of the screws.
The common denominator in all of the typical cases described is a dual guidance system using CT and fluoroscopy to facilitate positioning of the trocar by better visualisation of vertebral structures and lesions to be treated as well as to monitor vertebral filling in real time to limit cement leaks (13-14). These procedures are performed in a dedicated interventional CT suite under conditions of surgical asepsis. Preparation of the equipment necessitates: a sterile table drape, a sterile perforated drape (used for angioplasties), a 22-gauge needle for subcutaneous anaesthesia, a bottle of 1% xylocaine (lidocaïne 1% Xylocaïne; Astra, Sodertalge, Sweden), a scalpel and two 13-gauge trocars for guided vertebroplasty and vertebral biopsy (t’am,Thiebaud, Thonon-les-Bains, France).
Radiopaque markers were put on the skin prior to the insertion of the hardware. Using a 20-gauge 20-cm Shiba needle (Cook Medical, Bloomington, IN, USA), local anesthesia (lidocaïne 1% [Xylocaïne; Astra, Sodertalge, Sweden]) was administered from subcutaneous tissues to bone contact under fluoroscopy guidance according to the angle previously determined. A CT acquisition confirmed the correct positioning of the tip of the needle: a transpedicular approach is performed for the percutaneous screw fixation.
This needle was then used as a guide for a 13-gauge 10-cm Trocar t’am (Thiebaud, Thonon-les-Bains, France) which was inserted under fluoroscopy after the hub had been removed.
Using fluoroscopy guidance, the Trocar perpendicularly transfixed the acetabular fracture line. A follow-up via axial CT scans (SmartStep system) confirmed the good progression of the Trocar which was stopped immediately before perforating distal cortex. In case of pain, a Shiba needle was inserted inside the cannula to infuse 1 cc of lidocaïne 1%. A 2.0 mm Kirschner guidewire (Synthes, West Chester, PA, USA) was placed through the cannula (FIG 2).
Following the withdrawal of the cannula , a 4-mm cannulated self-drilling/tapping screw (Asnis III; Stryker, Mahwah, New Jersey, United States) was placed over the Kirschner guidewire under fluoroscopy guidance. Screw fixation was performed using a hollow screwdriver . The correct length of the screw was estimated by measuring the distance between the proximal and distal cortices on the axial CT images. Once the good positioning of the screw was confirmed by a CT scan, the guidewire was withdrawn .
A CT scan was performed at the end of the procedure to confirm the correct fixation of the fracture and eliminate any locoregional complication.
A contro-lateral approach is perform for the vertebroplasty. Monitoring by CT in step-by-step mode is used to confirm proper positioning of the Chiba needle. A further 3 cc (approximately) of 1% xylocaine is injected at the vertebral entry point to induce anaesthesia of the periostium. The break-off end of the Chiba needle is withdrawn, leaving space for a true guide, into which the perforated trocar (Trocar t’am (Thiebaud, Thonon-les-Bains, France) ) is inserted as far as bone contact and in particular the precise level of the anaesthesia . The advance of the trocar into the vertebral body is performed under iterative fluoroscopic and CT guidance . Proper final positioning of the distal end of the trocar in the fracture to be treated can be confirmed by CT monitoring. The CT guidance allowed a perfect visualization of the screw placed on the contralateral pedicle (FIG 3). The cement is prepared by means of the closed-loop mixer, in order to avoid vapour releases. The 1-cc Luer Lock syringes are filled with cement in its early liquid phase. We use a radio-opaque cement (Osteo-firm Radiopaque bone cement; Cook, Bloomington, IN, USA) in which we mix 4 grams of tungsten to make it highly radio-opaque. This high radio-opacity makes visualization perfect during vertebral filling, thus constituting an additional safety element(FIG 4-6) .
Follow-up
The post-operative follow-up which was performed by an independent assessor, an orthopaedic surgeon, ranged from 6 to 24 months. At each visit, plain radiographs and CT scan were performed.
Results
Six men and 4 women aged from 19 to 78 years (mean: 54 years) received this procedure. 5 had suffered traffic accidents, 1 falls from horseback, 4 skiing accidents. 5 at level L1, 3 at level L2 and 2 at level T12.
The mean interval between the injury and combined vertebroplasty and percutaneous screw fixation was 14 days (range, 2 – 30 days).
For each patient, one screw was inserted to fix the fracture. The mean length of screws was 38 mm (range, 22 mm – 55 mm). In all cases, screws were successfully placed in only one attempt (i.e., without intra-canalar penetration and cortical perforation). The mean procedure time was 45 min (range, 30 min – 90 min). The intervention was well tolerated by patients. No hemorraghe was observed.They were hospitalized for 48 hours in the department of orthopedic surgery. Physiotherapy was started on the first postoperative day with continuous passive motion. Assisted active range of motion and isometrical exercises were initiated on the second postoperative day. The cement volume injected varied betwenn 2cc to 5cc (m:2.8).DLP varied between 500 to 1620 microGy.cm3 (m:827)
The results obtained match those of the literature in the area of hyperalgesic osteopoenic fractures: The visual analogue scale and Oswestry disability index decreased from 8.2 +/- 1.6 to 2.5 +/- 1.4 and from 70.3 +/- 22.2 to 20.1 +/- 7.0 respectively. All of the results were stable in time and in particular over the long term at 6 months and 2 years. In all cases, CT monitoring revealed satisfactory consolidation of the fracture line. Follow-up CT imaging showed evidence of fracture healing. No superficial or deep infection occurred. No evidence of secondary displacement of the fragments, degenerative changes, screw failure or lucency adjacent to screws was noted. No heterotopic ossification was also observed.
Discussion
The results of our study showed that Split-burst fractures could be successfully treated by percutaneous screw fixation under CT and fluoroscopy guidance with an excellent long-term outcome. This technique of percutaneous fixation was first described by Gay et al. in 1992 [12]. In their report they showed that it offered several advantages over open reduction and internalfixation. First, soft-tissue disruption with the potential for devascularization or denervation is virtually eliminated. Blood loss is also significantly decreased, and a lower risk of infection may be anticipated owing to decreased tissue trauma and the lack of an open wound. Second, functional recovery was improved: patients could begin more rapidly weight-bearing, avoiding decubitus complications Third, CT scans were useful to evaluate the severity and geometry of the fractures. Three-dimensional reconstructions were also used to plan fixation procedure.
Vertebroplasty for split burst fracture is a delicate procedure in many aspects. The fracture separates the vertebral wall into 2 parts and may cause collapse of the posterior wall. This procedure is still within the limits of the indications of vertebroplasty, but the decision to proceed must be made in agreement with the neurosurgical or orthopaedic team. In our experience, the coupling of CT and fluoroscopy is fundamental. The axial slices permit perfect visualization of the ends of the trocars precisely within the vertebral fracture. The fluoroscopic guidance verifies that the trocars are at mid-height of the vertebra. The trocars are advanced successively under monitoring by CT slices and lateral fluoroscopy. We use 13-gauge trocars and insert them manually. We also avoid the use of a surgical hammer, so as to limit the risk of displacement of bone fragments. We transfix the fracture line with the two trocars in bilateral and symmetric manner, with their ends situated medially in order to limit lateral leaks.In one side we insert the screw, in the other side we perform the vertebroplasty. While in its pasty phase, the cement is injected at the level of the anterior fragment of the fracture, then the trocar is withdrawn very slowly to the fracture level while cement is injected progressively, in order to create a cement bridge between the anterior fragment and the fracture line. A CT control verifies that the end of the trocar is situated perfectly in the fracture. The cement is injected slowly into the cannula then pushed with the needle of the trocar. The diffusion of the cement into the fracture line in real time is monitored by lateral fluoroscopy. The axial CT slices confirm the good diffusion into the fracture and the absence of para-vertebral leaks.
In our study, percutaneous fixation performed only under local anesthesia was guided by the combination of CT and fluoroscopy. Gangi et al. [13] showed in vertebroplasty procedures that this dual guidance could allow to facilitate needle placement and reduce complications. The traditional treatment of this type of fracture is either conservative, involving the wearing of a corset, or surgical, with posterior arthrodesis(14-17). These two techniques have their own disadvantages in terms of consolidation time and risk of pseudarthrosis as well as postoperative risks of infection or functional impairment due to attack of the para-vertebral muscle masses and of the presence of the arthrodesis material. Vertebroplasty offers an intermediate alternative to the traditional treatments. Percutaneous vertebroplasty is a vital procedure in the therapeutic arsenal for vertebral fractures. The crucial role of dual guidance, which made the intervention rapid, safe and effective, was confirmed in various percutaneous interventions including fixation of vertebral pedicle fractures [14]
Moreover, the hardware used in this procedure is available in most hospitals where orthopedic surgery is performed. We attribute the absence of complications with this technique to the fact that insertion of the screws is technically easy under CT and fluoroscopy guidance, and the learning curve, therefore, is short. The good reproducibility of this technique was also strongly suggested by Gay .
Lastly, the follow-up of our patients showed an excellent long-term outcome with a functional recovery which was not affected by the occurrence of hip degenerative changes.
Our study showed the accuracy of combined vertebroplasty and percutaneous screw fixation to treat vertebral split burst fracture.
2. Franc J, Lehmann P, Saliou G, Monet P, Kocheida EM, Daguet E, Laurent A, Legars D, Deramond H. Vertebroplasty: 10 years clinical and radiological follow-up.J Neuroradiol. 2010 Oct;37(4):211-9
3. Fransen H. Minimal invasive treatment of vertebral compression fractures: vertebroplasty.Neuroradiology. 2011 Sep;53 Suppl 1:S199-201.
4. Muijs SP, van Erkel AR, Dijkstra PD. Treatment of painful osteoporotic vertebral compression fractures: a brief review of the evidence for percutaneous vertebroplasty.J Bone Joint Surg Br. 2011 Sep;93(9):1149-53
5. Klazen CA, Lohle PN, de Vries J, Jansen FH, Tielbeek AV, Blonk MC, Venmans A, van Rooij WJ, Schoemaker MC, Juttmann JR, Lo TH, Verhaar HJ, van der Graaf Y, van Everdingen KJ, Muller AF, Elgersma OE, Halkema DR, Fransen H, Janssens X, Buskens E, Mali WP. Vertebroplasty versus conservative treatment in acute osteoporotic vertebral compression fractures (Vertos II): an open-label randomised trial.Lancet. 2010 Sep 25;376(9746):1085-92
6. Brodano GB, Amendola L, Martikos K, Bettuzzi C, Boriani L, Gasbarrini A, Bandiera S, Terzi S, Greggi T, Boriani S. Vertebroplasty: benefits are more than risks in selected and evidence-based informed patients. A retrospective study of 59 cases.Eur Spine J. 2011 Aug;20(8):1265-71
7. Anselmetti GC, Manca A, Montemurro F, Hirsch J, Chiara G, Grignani G, Carnevale Schianca F, Capaldi A, Rota Scalabrini D, Sardo E, Debernardi F, Iussich G, Regge D.Percutaneous vertebroplasty in multiple myeloma: prospective long-term follow-up in 106 consecutive patients.Cardiovasc Intervent Radiol. 2012 Feb;35(1):139-45 2012
8. Saliou G, Kocheida el M, Lehmann P, Depriester C, Paradot G, Le Gars D, Balut A, Deramond H. Percutaneous vertebroplasty for pain management in malignant fractures of the spine with epidural involvement.Radiology. 2010 Mar;254(3):882-90.
9. Lee B, Franklin I, Lewis JS, Coombes RC, Leonard R, Gishen P, Stebbing J.The efficacy of percutaneous vertebroplasty for vertebral metastases associated with solid malignancies.Eur J Cancer. 2009 Jun;45(9):1597-602
10. Mont’Alverne F, Vallée JN, Guillevin R, Cormier E, Jean B, Rose M, Caldas JG, Chiras J.Percutaneous vertebroplasty for multiple myeloma of the cervical spine.Neuroradiology. 2009 Apr;51(4):237-42
11. McDonald RJ, Trout AT, Gray LA, Dispenzieri A, Thielen KR, Kallmes DF. Vertebroplasty in multiple myeloma: outcomes in a large patient series.AJNR Am J Neuroradiol. 2008 Apr;29(4):642-8. Epub 2008
12. Gay SB, Sistrom C, Wang GJ, Kahler DA, Boman T, McHugh Net al
(1992) Percutaneous screw fixation of acetabular fractures with
CT guidance: preliminary results of a new technique. AJR
American Journal Roentgenology 158:819–822
13. Gangi A(1994) Percutaneous vertebroplasty guided by a combination of CT and fluoroscopy.AJNR. Am J Neuroradiol. 15(1):83-6.
14. Schmid R, Lindtner RA, Lill M, Blauth M, Krappinger D. Combined posteroanterior fusion versus transforaminal lumbar interbody fusion (TLIF) in thoracolumbar burst fractures.Injury. 2012 Jan 6
15. Schmid R, Krappinger D, Seykora P, Blauth M, Kathrein A. PLIF in thoracolumbar trauma: technique and radiological results.Eur Spine J. 2010 Jul;19(7):1079-86
16. Rajasekaran S.Thoracolumbar burst fractures without neurological deficit: the role for conservative treatment.Eur Spine J. 2010 Mar;19 Suppl 1:S40-7
17. Blondel B, Fuentes S, Metellus P, Adetchessi T, Pech-Gourg G, Dufour H.Severe thoracolumbar osteoporotic burst fractures: treatment combining open kyphoplasty and short-segment fixation.Orthop Traumatol Surg Res. 2009 Sep;95(5):359-64
18. Amoretti N, Marcy PY, Hauger O, Browaeys P, Amoretti ME, Hovorka I, Boileau P. Percutaneous screw fixation of a vertebral pedicle fracture under CT-guidance : A new technique. Eur J Radiol. 2011
Captions for figures[/toggle]